












A Scoping Review of Japanese Dance/Movement Therapy Intervention Studies
Volume 11, Issue 2, Pages 320-346
Abstract
This study presents the first literature review of dance/movement therapy (DMT) intervention studies conducted in Japan using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews. It aims to examine participants, outcome measures, intervention methods, effects, and study quality. Searches were conducted using Japanese databases, including Ichushi, CiNii, and Medical-Online, and English databases, including PubMed and Google Scholar, along with the Japanese Journal of Dance Therapy and the American Journal of Dance Therapy. Nine studies met the inclusion criteria. Findings revealed the following: levels of evidence: level 2, two studies; level 3, three studies; level 4, four studies; most common participants: individuals with intellectual disabilities (n=42, 24.8%); 13 (35.1%) of 37 outcome measures were standardized or objective; most used intervention: structured (n=5, 50.0%); frequent effects: improved balance and positive expression (both n=3, 13.0%).
摘要
本研究采用“系统评价和荟萃分析首选报告项目范围综述扩展版”(Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews,简称PRISMA-ScR),对日本开展的舞蹈/动作治疗(Dance/Movement Therapy,DMT)干预研究进行了首次文献综述。其目的在于对参与者、结局指标、干预方法、干预效果及研究质量进行分析。检索范围包括日文数据库 (Ichushi、CiNii、Medical-Online)、英文数据库 (PubMed、Google Scholar), 以及《日本舞蹈治疗杂志》和《美国舞蹈治疗杂志》。最终,共有九项研究符合纳入标准。研究发现如下:证据等级:2级(两项研究);3级(三项研究);4级(四项研究);最常见的参与者:智力障碍人士(n=42,占24.8%);在37项结局指标中,有13项(35.1%)采用标准化或客观测量工具;最常用的干预形式:结构化干预(n=5,占50.0%);常见效果:平衡能力改善与积极情绪表达(均为n=3,各占13.0%)。
Keywords
dance/movement therapy, PRISMA-ScR, levels of evidence, intellectual disability.
关键词
舞蹈/动作治疗, PRISMA-ScR, 证据等级, 智力障碍.
History
Received 01 April 2025
Accepted 01 June 2025
Open Access
This is an open access article.
Background
According to the American Dance Therapy Association (ADTA, 2020), dance/movement therapy (DMT), also known as dance therapy, is defined as “the psychotherapeutic use of movement to promote emotional, social, cognitive, and physical integration of the individual, for the purpose of improving health and well-being.” DMT can provide mental, behavioral, and physical treatment through body and mind connections (Levy, 2005).
ADTA, established in 1966, is one of the most historic DMT associations (Ohnuma et al., 2012). The Japan Dance Therapy Association (JADTA) was established in 1992, 26 years after ADTA was established (Ohnuma et al., 2012).
The JADTA indicates that “there is no clear definition” of DMT in Japan (Ohnuma et al., 2012). However, Ohnuma et al. (2012) stated that Japanese DMT refers to psychological treatment using techniques of movement and dance that aim to improve the maintenance, promotion, and restoration of mental and physical health.
In 1999, the JADTA began offering dance therapist certification to those who met certain criteria as private qualifications, and in 2004, it began offering training sessions for those wishing to become certified by the association (Ohnuma et al., 2012). In 2006, as an additional certification, the JADTA included the Associate Dance Therapist certification and Dance Therapy Leader certification, which is the foundational certification for dance therapists (Ohnuma et al., 2012). Since then, three types of dance therapy certification have existed in Japan.
To become a dance therapist in Japan, the following requirements should be met: 60-credit certification course; minimum of 100 hours of experience in modern dance and other dance styles; minimum of 200 hours of clinical experience with any master’s degree; passing the final practical examination; membership in the association for at least 3 years; attending at least two annual conferences; presence in at least one annual conference (JADTA, 2008).
In 2011, JADTA reported 25 certified dance therapists, four associate dance therapists, and 146 dance therapy leaders (Ohnuma et al., 2012). In 2023, the annual conference of the JADTA reported 32 certified dance therapists, three associate dance therapists, and 591 dance therapy leaders (JADTA, 2023).
DMT is performed in three main areas of Japan: medical facilities, such as hospitals and clinics; welfare areas, such as facilities for the elderly and those with disabilities and disorders; educational facilities, such as preschools, kindergartens, universities, and dance studios (Ohnuma et al., 2012).
Since the establishment of the JADTA, interventional studies have been conducted on individuals with several types of disabilities and disorders (Ohnuma et al., 2012). Positive effects of DMT practices in Japan have been reported, such as improved self-awareness and awareness of others in individuals with intellectual disability (Mukaide, 2020), and increased feelings of joy in individuals with schizophrenia spectrum disorder (Ohno, 2014).
Although there have been reports of some positive effects of DMT practices on several disorders and diseases, no studies have integrated and characterized Japanese DMT intervention studies, including the main targets, intervention methods, and effects of DMT intervention studies.
In the clinical practice of DMT in Japan, it is important to clarify the characteristics and trends of DMT intervention studies to clarify treatment effects in clinical situations. Clarifying the characteristics of these DMT intervention studies and trends in treatment effects in Japan will contribute to the development of DMT as a treatment not only in Japan but also in Asia.
This study aimed to identify and review the literature regarding the DMT intervention studies in Japan and synthesize information relating to the current status of DMT intervention studies in Japan.
To achieve the study’s aims, the following research questions are stated:
Who is the target population for DMT intervention studies in Japan, such as age, sex, and diseases or disorders?
What are the outcome measures of the DMT intervention studies in Japan?
What are the methods of DMT interventions in Japan?
What is the effectiveness of DMT interventions in Japan?
What are the quality and levels of evidence (LOEs) of DMT intervention studies in Japan?
Methods
In this study, only previously published studies were reviewed. Therefore, additional formal ethics committee approval or informed consent was not required.
Scoping Review
A scoping review is a summary of the key concepts underlying an area of research, the main sources of information, and the types of literature and information available, and its purpose is to examine the breadth, scope, and nature of research activity (Arksey & O’Malley, 2005). The purpose of conducting the scoping review in this study is to provide a comprehensive overview of the wide range of findings on the current state of DMT in Japan.
This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) (Tricco et al., 2018) and adhered to the PRISMA-ScR Checklist.
Selection Criteria
In this study, the scoping review was conducted in stages, with additional investigations carried out based on the findings from the initial review. The first investigation was conducted from January 9, 2022, to February 9, 2022. Subsequent additional searches were performed from December 24 to 31, 2023, August 8 to 9, 2024, and February 28 to March 3, 2025.
The survey was conducted in both Japanese and English. The Japanese survey covered the period from 1992, when JADTA was established, to March 3, 2025, whereas the English survey covered the period from 1966, when ADTA was established, to March 3, 2025.
Searches were conducted using the Japanese search engines, such as Ichushi, CiNii, and Medical-Online, and the English search engines, including PubMed and Google Scholar. Predefined search terms were used for each database. The Japanese Journal of Dance Therapy and the American Journal of Dance Therapy were identified as major DMT journals.
The search key terms were combined as “dansu/mūbumento serapi” (dance/movement therapy) or “dansu serapi” (dance therapy) and “kainyu-kenkyu” (intervention study), “Jissen” (practice), or “Kouka-kenkyu” (effective study). To specify Japanese DMT in the search, the search key terms “Japanese dance/movement therapy” or “Japanese dance therapy” were used in the English search.
After removing 31 duplicate references from the initial screening, titles and abstracts were screened based on the acceptance criteria.
Literature extraction was verified multiple times by the authors, after which all the selected studies were carefully reviewed to evaluate the inclusion and exclusion criteria. If any disagreements arose during the screening process, the authors discussed and made a final decision. The selected Japanese studies were translated into English by the authors, and proofread by an English proofreader.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: original research articles published in academic journals in either Japanese or English in the period covered by the survey; using DMT interventions; using an intervention study design; texts including information that the DMT intervention was conducted in Japan, such as the fact that the participants were recruited in Japan or the description of the place of implementation of the DMT intervention in Japan.
The exclusion criteria were studies published in languages other than Japanese or English and articles published as meta-analyses, systematic reviews, narrative reviews, research notes, research and clinical reports, short and any other reports, special issues, theses, articles in books, and articles using interventions other than DMT. Studies using the DMT program as part of college or school coursework were excluded because the therapeutic effect of DMT was unknown. The introduction of the journal and the congratulatory addresses in the first issue were also excluded.
Levels of Evidence
The selected studies were evaluated to clarify their quality and evidence using LOE assessment tools developed by the Oxford Centre for Evidence-Based Medicine in 2011 (Centre for Evidence-Based Medicine, 2022).
LOE is designed to allow clinicians and patients to rapidly answer clinical questions and find feasible evidence (Center for Evidence-Based Medicine, 2022). It is structured into five levels, with level 1 indicating the highest quality of evidence and level 5 representing the lowest (Center for Evidence-Based Medicine, 2022).
Results
Search Results
The initial search identified 672 studies and excluded 31 duplicates. The numbers of studies identified in each database were as follows: Ichushi, n=14; CiNii, n=35; Medical-Online, n=9; Google Scholar, n=15; PubMed, n=3. The results of additional records identified from other sources were as follows: Japanese Journal of Dance Therapy, n=81; American Journal of Dance Therapy, n=515.
During the first screening, the results were refined using specific key terms in the titles and abstracts of journals, eliminating 600 studies. Subsequently, during the full-text article assessment, the selected studies were reviewed to determine whether they satisfied the inclusion criteria.
A total of 63 studies were excluded from the analysis. The most common database search and additional search sources for the excluded studies were the Japanese Journal of Dance Therapy (n=32, 50.7%) and CiNii (n=19, 30.1%). The most common studies among the excluded studies were based on clinical reports (n=14, 27.4%), followed by special issues (n=13, 25.4%). Finally, nine studies satisfied the requirements (Arakawa, 2000; Ishikawa et al., 2014; Kaji et al., 2000; Kozuka & Chino, 2008; Shiba & Tanaka, 1993; Takahashi et al., 2020, 2022, 2023; Watanabe et al., 2011). The selected studies were analyzed during the final screening (Figure 1).
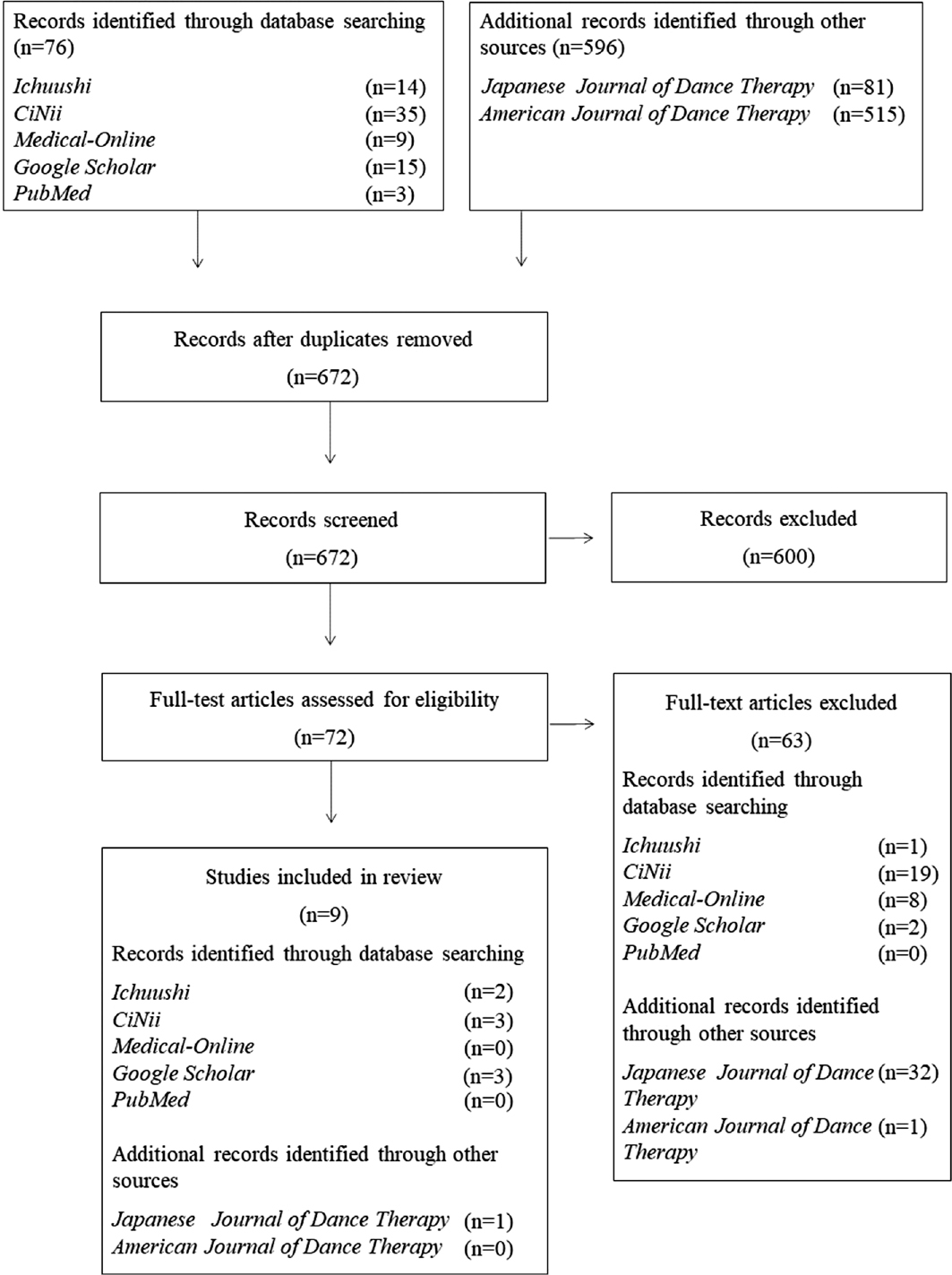
Figure 1 - Study flow diagram.
The selected studies were classified into 12 categories for data analysis: authors, years, study design, objects, participants (number of participants, sex, age or mean age±standard deviation, age range, and types of disease or disorder), session format (individual or group), methods (session duration, frequency, and number of sessions), interventions, elements of activities in the interventions, main outcome measures, results of the study, and conclusions (Table 1). The study design was classified following Tsushima (2017).
Authors | Years | Study design | Objective | Participants: (1) Number of participants (2) Sex (males/females) (3) Age or mean age±standard deviation (years) (4) Range of age (years) (5) Types of disease or disorder | Session format (individual or group) | Methods: (1) Session duration (2) Frequency (3) Number of sessions | Interventions | Elements of activities in the interventions | Main outcome measures | Results of the study | Conclusions |
|---|---|---|---|---|---|---|---|---|---|---|---|
Shiba & Tanaka | Case series study | Investigate the practice and the evaluation of the DMT practiced with the psychiatric inpatients in the purpose of the creative self-expression | (1) 2 participants (2) 0:2 (3) 33 and 42 (4) 33 and 42 (5) Personality disorder, schizophrenia spectrum disorder | Group session | (1) 60 minutes (2) Once in 2 weeks (3) More than 19 times | (1) Folk dance (2) Research on various ways of movement of body (3) Expression challenge (4) Individual presentation (5) Summary of activity including feedback | (1) Breathing and movement (2) Expressing own image (3) Holding the hands and dance together (4) Presenting own dance to other participants | (1) Observing movements through recorded video (2) Interview | (1) Improving feeling the pleasure of creating self-expression (2) Improving empathy through the dance of other participants (3) Improving the non-verbal communication skills | DMT interventions helped to improve a temporary positive effect on self-expression and behavioral aspects of patients such as non-verbal communication and empathizing with others | |
Arakawa | Case series study | Investigate the effectiveness of DMT for patients with dementia | (1) 9 participants (2) 2:7 (3) 76±unknown (4) 60 to 85 (5) Alzheimer disease for 4 participants, vascular dementia for 3 participants, dementia with a psychiatric disorder for 1 participant, and dementia in head injury for 1 participant | Group session | (1) 45 to 60 minutes (2) Once in 2 weeks (3) 6 times | (1) Pre-warm up (2) Warm-up (3) Development (main activity with themes) (4) Close | (1) Breathing (2) Holding the hands and rubbing the hands (3) Massaging (4) Mirroring (5) Singing 6) Using percussion instruments | (1) Observing movements through recorded video (2) Self-generated evaluation chart with reference to N-shiki-rounensha-you-seishin-shakudo (NM scale) (Mental Status Scale for the Elderly) (3) Self-generated physical exercise assessment | (1) Improving reminiscing activities (2) Improving social skills | DMT intervention helped patients with several types of dementia to improve reminiscing activities and social skills | |
Kaji et al | Before-after trials | Investigate the efficacy of DMT through a quantitative evaluation that utilizes empirical and scientific methodology | First research (1) 70 participants (2) 6:64 (3) 22.0±unknown (4) Unknown (5) Healthy individual Second research (1) 31 participants (the number of valid respondents used for data analysis was 26 participants) (2) 10:16 (3) 34.6±unknown (4) Unknown (5) Schizophrenia spectrum disorder for 15 participants, manic-depressive disorder for 3 participants, eating disorder for 3 participants, borderline personality disorder for 2 participants, avoidant personality disorder for 2 participants, depressive disorder for 1 participant | Group session: first research Group session: Second research | First research (1) 45 minutes (2) Unknown (3) Unknown Second research (1) 45 minutes (2) Unknown (3) Unknown | (1) Unknown for both research | First research (1) Unknown Second research (1) Choreography (2) Imaginary dance (3) Movements with non-verbal communication | First research (1) Jikoninchi-shakudo (Self-Cognitive Scale) (2) Shintaizou-shakudo (Body Image Scale [SD method on a seven-point scale]) (3) Draw-a-Person method Second research (1) Jikoninchi-shakudo (Self-Cognitive Scale) (2) Shintaizou-shakudo (Body Image Scale [SD method on a seven-point scale]) (3) Draw-a-Person method (4) Brief Psychiatric Rating Scale | First research (1) Significant differences were found in all items of the self-cognitive scale (p<.000) (2) Body image changed from negative to positive (3) Post-therapy drawings showed significantly more portraits of people with bright expressions (p<.01), arms outstretched (p<.01), people in motion (p<.01), and people looking forward (p<.05). After the therapy, the portraits were drawn significantly larger (p<.05) Second research (1) Self-Cognitive Scale showed a significant difference (p<.00) (2) Body Image Scale showed a significant difference (p<.05) (3) Comparison of the two interventions, the body image for participants with healthy individual (participants in the first research) significantly improved (F1,1=6.06, p<.05) (4) All participants improved their scores of self-cognitive after DMT sessions in the Brief Psychiatric Rating Scale | DMT interventions helped to improve self-cognitive and body image of the participants | |
Kozuka & Chino | Case study | Investigate the effectiveness of DMT as a method of the early development supports for 10 years old boy with autism spectrum disorder | (1) One participant (2) 1:0 (3) 10 (4) – (5) Autism spectrum disorder with intellectual disability | Individual session | (1) 40 minutes (2) Unknown (3) 10 times | (1) Unknown | (1) Jumping (2) Moving to music (3) Touching | (1) Observing movements through recorded video | (1) Improved positive face during the session Positive faces were observed 41 times, whereas negative faces were observed 13 times (2) Improved empathy with others | DMT interventions help patients show more positive facial expressions, defined as “positive faces,” than negative facial expressions, described as “negative faces,” and empathy for others | |
Watanabe et al | Controlled clinical trial without RCTs | Investigate the psycho-physiological effects of group DMT interventions for frail elderly women with diseases or disabilities | Intervention group (1) 11 participants (2) 0:11 (3) Unknown for intervention group (4) Unknown for intervention group (5) Parkinson disease for 3 participants, sequelae of brain disease for 3 participants, depression disorder for 2 participants, diabetes mellitus disease for 1 participant, chronic pneumonia disease for 1 participant, osteoporosis of the spine for 1 participant Control group (1) 11 participants (2) 0:11 (3) Unknown for control group (4) Unknown for control group (5) Sequelae of brain disease for 3 participants, diabetes mellitus disease for 3 participants, angina pectoris disease for 2 participants, lumbar spinal canal stenosis for 1 participant, lumbosacral caries for 1 participant, Alzheimer disease for 1 participant (mean of age of both groups, 78.7±7.3 years; range of both groups, 66–95 years) | Group session | (1) 60 minutes (2) Once a week (3) 10 times | (1) Unknown | (1) Breathing (2) Rhythmic aerobic dance (3) Shifting weight or standing on one leg stand (4) Slowly dance on standing position (5) Stretching 6) Touching 7) Turning over or standing up from sitting position slowly | (1) Percentage of heart rate reserve (% HRR) (2) Face Scale (Emotional State Test) (3) Saliva levels of the stress-related hormones cortisol and chromogranin A | (1) Average HRRs in the intervention and control groups: 13.1%±1.3% and 12.1%±1.6%, respectively (2) Improved emotional well-being (p<.05) Cortisol and chromogranin A did not change | Short DMT interventions seem no to provide physical stress to the participant and might help to improve the emotional well-being for the participants | |
Ishikawa et al | RCTs | Investigate the effectiveness of the DMT interventions for elderly participants with dementia using the measurements of cognitive function, behavioral psychological symptoms of dementia, and activities of daily living. Moreover, investigate the effectiveness of brain function and neurophysiological effects | Intervention group (1) 9 participants (2) 2:7 (3) 82.4±7.5 (4) Unknown for intervention group (5) Alzheimer disease for 3 participants, Mixed dementia of Alzheimer and vascular for 2 participants, dementia with Lewy bodies for 2 participants, Parkinson disease with dementia for 1 participant, frontotemporal dementia for 1 participant Control group (1) 9 participants (2) 2:7 (3) 77.6±11.6 (4) Unknown for control group (5) Alzheimer disease for 5 participants, vascular dementia for 2 participants, dementia with Lewy bodies for 1 participant, Parkinson disease with dementia for 1 participant | Group session | (1) 30 to 40 minutes (2) Once a week (3) 8 times | (1) Introduction (2) Development (3) Close | (1) Authentic movement (2) Massaging (3) Mirroring (4) Pair dancing (5) Self-touching | (1) Mini-Mental State Examination (MMSN) (2) Verbal fluency task (VFT) (3) Psychogeriatric Assessment Scale (PAS) (4) Neuropsychiatric Inventory (NPI) (5) N-shiki-rounensha-you-nichijou-seikatsu-dousa-nouryoku-hyoukashakudo (Activity of Daily Living Scale for Elderly) (N-ADL) (6) Nihon Kouden Nouhakei EEG-9100 (electroencephalograph) (7) Kan’igata Amylase Sokuteiki (salivary amylase activity monitor) | (1) Although the MMSN, VFT, PAS, NPI, and N-ADL did not show significant difference, the MMSE score tended to improve (r=.54) (2) Electroencephalography results showed no significant differences between the intervention and control groups. However, there was a significant trend in the first (0.12±0.08) and second (0.07±0.05) sessions of the intervention group (p=.051, r=.65) (3) Salivary amylase activity showed an increasing trend in values before and after the first four sessions and a decreasing trend in the latter part of the sessions. There was a significant difference between the first and second halves of the session (p<.05, r=−.90) | DMT interventions for the participants with dementia may benefit for their cognitive, brain, and independent neurological function | |
Takahashi et al | Case series study | Investigate the effectiveness of DMT for individuals with Williams syndrome | (1) 4 participants (2) 2:2 (3) 7±2.1 (4) 5 to 10 (5) Williams syndrome with intellectual disability | Group session | (1) 60 minutes (2) Once a week (3) 10 times | (1) Warm-up (2) Development (main activities) (3) Cool down | (1) Authentic movement (2) Laban movement analysis (3) Mirroring (4) Moving on balance balls and balance cushions (5) Stillness and gentle movement | (1) Wechsler Intelligence Scale (2) Posturography (static balance) (3) Hand-held dynamometer (lower limb muscle strengths) (4) Timed Up and Go (dynamic balance) (5) Child Behavior Checklist | (1) IQ range: 43–66 (2) Posturography showed that all participants decreased total sway length in eyes-open and eyes-closed conditions (3) Hand-held dynamometer results showed that all participants improved both right and left knee extensor muscles (4) Timed Up and Go showed that one participant decreased the time by 1.45 seconds but the other three participants did not show any major difference (5) Child Behavior Checklist showed that participants did not show any major difference | DMT interventions helped children with Williams syndrome to improve static balance and knee extensor muscles | |
Takahashi et al | Before-after trials | Investigate the effectiveness of DMT for individuals with intellectual disability | (1) 21 participants (2) 16:5 (3) 3.8±0.9 (4) 3 to 6 (5) Intellectual disability | Group session | (1) 60 minutes (2) Once a week (3) 10 times | (1) Warm-up (2) Development I (main activity I) (3) Development II (main activity II) (4) Cool down | (1) Authentic movement (2) Laban movement analysis (3) Mirroring (4) Synchronizing movements | (1) One-Leg Stand Test (OLST) (2) Timed Up and Go (dynamic balance) (3) Hand-held dynamometer (knee extensor muscles) (4) Child Behavior Checklist (5) Caregiver–Teacher Report Form | (1) OLST showed significant improvements in both the left (z=1.96 p=.036) and right (z=1.84, p=.033) legs (2) Timed Up and Go did not show a significant improvement (z=−0.42, p=.34) (3) Hand-held dynamometer measurements showed a significant improvement on the left (z=2.85, p=.002) and right (z=1.87, p=.031) legs (4) Child Behavior Checklist showed a significant decrease in attention (z=− 1.96, p=.025) and affective problems (z=−1.72, p=.043) (5) Caregiver–Teacher Report Form showed a significant decreased in total score (z=−2.76, p=.003), internalizing problems (z=−2.13, p=.017), externalizing problems (z=−2.49, p=.007), affective problems (z=−2.07, p=.020), anxiety problems (z=−1.74, p=.044), attention deficit/hyperactivity problems (z=−2.56, p=.005), and somatic complaints (z=−1.72, p=.043 | DMT intervention helped children with intellectual disability to improve static balance and knee extensor muscles, and decrease in attention and affective problems in child behavior checklist, and total score, internalizing problems, externalizing problems, affective problems, anxiety problems, and attention deficit/hyperactivity problems in the Caregiver–Teacher Report Form | |
Takahashi et al | RCTs | Investigate the effectiveness of DMT group intervention in individuals with Down syndrome | Intervention group (1) 16 participants (2) 10:6 (3) 12.94±6.55 (4) Unknown for intervention group (5) Down syndrome with intellectual disability Control group (1) 15 participants (2) 8:7 (3) 13.00±6.38 (4) Unknown for control group (5) Down syndrome with intellectual disability | Group session | (1) 60 minutes (2) Once a week (3) 10 times | (1) Warm-up (2) Development I (main activity I) (3) Development II (main activity II) (4) Cool down | (1) Authentic movement (2) Creating imagery movements dynamically (3) Efforts of Laban movement analysis (4) Improvisational movement (5) Mirroring 6) Share movement experiences or feeling of the session 7) Stillness and gentle one’s own inner movements on sitting position 8) Synchronizing movements 9) Using balance cushion | (1) Wechsler Intelligence Scale (2) Posturography (Static balance) (3) Timed Up and Go (dynamic balance) (4) Achenbach System of Empirically Based Assessment (Adult Behavior Checklist, Child Behavior Checklist and Teacher Report Form [TRF]) | (1) The mean IQ in the intervention group was 42.67±2.87 and 42.71±2.52 in the control group (2) Posturography in the eyes-open condition did not show any significant difference in total length (F=0.51, p=.48, ηp2=0.02), root mean square mediolateral (F=1.28, p=.27, ηp2=0.04), and root mean square anteroposterior (F=0.31, p=.58, ηp2=0.01) Posturography in the eyes-closed condition did not show any significant difference in total length (F=0.02, p=.90, ηp2=0.00), root mean square mediolateral (F=2.59, p=.12, ηp2=0.09), and root mean square anteroposterior (F=0.00, p=.98, ηp2= 0.00) (3) Timed Up and Go results showed a significant improvement (F=4.53, p=.04, ηp2=0.14) The intervention group showed a significant improvement (p=.00); however, the control group did not show a significant difference (p=.85) (4) The results of the Adult Behavior Checklist and Child Behavior Checklist did not show any significant difference in total score (F=0.20, p=.66, ηp2=0.01), internalizing problem (F=0.69, p=.41, ηp2=0.02), and externalizing problems (F=0.05, p=.82, ηp2=0.00) Moreover, the TRF did not show any significant difference in total score (F=2.17, p=.17, ηp2=0.17), internalizing problem (F=0.74, p=.41, ηp2=0.06), and externalizing problems (F=4.19, p=.07, ηp2=0.28) | DMT intervention helped individuals with Down syndrome to improve the dynamic balance after the 10 times of once a week DMT session |
Characteristics of DMT Participants
Nine studies were selected, one of which involved two intervention studies (Kaji et al., 2000). In studies in which age was explicitly reported (n=8, 80.0%), participants’ ages ranged from 3 to 85 years. The mean ages of the most frequent participants were younger than 10 years (n=2, 25.0%), between 10 and 20 years (n=2, 25.0%), and older than 76 years (n=2, 25.0%).
The participants for DMT interventions were diagnosed with the following 24 diseases or disorders: Alzheimer disease, autism spectrum disorder with intellectual disability, avoidant personality disorder, borderline personality disorder, chronic pneumonia disease, dementia with Lewy bodies, dementia in head injury, dementia with a psychiatric disorder, depressive disorder, diabetes mellitus disease, Down syndrome with intellectual disability, eating disorder, frontotemporal dementia, intellectual disability, manic-depressive disorder, mixed dementia of Alzheimer and vascular, osteoporosis of the spine, Parkinson disease, Parkinson disease with dementia, personality disorder, schizophrenia spectrum disorder, sequelae of brain disease, vascular dementia, and Williams syndrome with intellectual disability. Healthy individuals participated in the DMT intervention study.
The total number of DMT intervention participants was 169, of whom 99 (58.5%) had some type of disease or disorder. Seventy (41.4%) participants were healthy.
The most common disease or disorder for DMT interventions in Japan was intellectual disability in four studies (44.4%), with a total of 42 participants (24.8%). Among the 42 participants with intellectual disability, one had autism spectrum disorder (2.3%), 16 had Down syndrome (38.0%), and four had Williams syndrome (9.5%). Other DMT participants were individuals with intellectual disability with no other complications (n=21, 50.0%). The second most common disease or disorder was schizophrenia spectrum disorder, which was observed in two studies (22.2%) with a total of 16 participants (16.1%).
Characteristics of Outcome Measures
Thirty-seven outcome measures were conducted, of which the most common were the Child Behavior Checklist (n=3, 8.1%), observing movements through recorded videos (n=3, 8.1%), and Timed Up and Go (n=3, 8.1%). The same researchers (Takahashi et al., 2020, 2022, 2023) used the Child Behavior Checklist and Timed Up and Go in separate studies.
The next most common outcome measures were Caregiver–Teacher Report Form (n=2, 5.4%), Draw-a-Person method (n=2, 5.4%), hand-held dynamometer (n=2, 5.4%), Jikoninchi-Shakudo (Self-Cognitive Scale) (n=2, 5.4%), posturography (n=2, 5.4%), Shintaizou-Shakudo (Body Image Scale) (n=2, 5.4%), and Wechsler Intelligence Scale (n=2, 5.4%). The Caregiver–Teacher Report Form (Takahashi et al., 2022, 2023), hand-held dynamometer, posturography, and Wechsler Intelligence Scale (Takahashi et al., 2020, 2022) were used by the same researcher in separate studies. The Jikoninchi-Shakudo (Self-Cognitive Scale) and Shintaizou-Shakudo (Body Image Scale) were used by the same researcher (Kaji et al., 2000) to evaluate the two interventions in one study.
Of the 37 outcome measures, only 13 (35.1%) were standardized or objective. Of these, six (16.2%) were standardized assessments, including the following: The Achenbach System of Empirically Based Assessment, including an Adult Behavior Checklist for Adults and the Elderly, Child Behavior Checklist for Young and School-Age Children, and Teacher Report Form for Young and School-Age Children (Achenbach, 2015), which are checklists that provide evidence-based assessments that assess the participants’ adaptive function and behavioral, emotional, and social problems (Achenbach, 2015); Brief Psychiatric Rating Scale for assessing the participants’ psychiatric symptoms such as depression, anxiety, and unusual behavior (Overall & Gorham, 1962); Mini-Mental State Examination for quantitatively estimating the degree of cognitive impairment and continuously documenting the changes in cognitive function (Molloy et al., 1991; Tombaugh & Mclntyre, 1992); Neuropsychiatric Inventory for assessing the participants’ behavioral psychological symptoms of dementia (Kaufer et al., 1998); Psychogeriatric Assessment Scale used for assessing the clinical changes seen in dementia and depression (Jorm et al., 1997); Wechsler Intelligence Scale for assessing the participants’ intelligence quotient (Keith et al., 2006; Tulsky et al., 2001).
Seven studies (18.9%) used objective measures, including hand-held dynamometer for assessing the participants’ muscle strengths (Stark et al., 2011); heart rate reserve for assessing the participants’ percentage of heart rates (Swain & Leutholtz, 1997); Kan’igata Amylase Sokuteiki (salivary amylase activity monitor) for assessing the participants’ salivary amylase activity levels (Yamaguchi et al., 2004); Nihon Kouden Nouhakei EEG-9100 (electroencephalography) for assessing the participants’ electroencephalograms (Çabalar et al., 2011); physiological indicator of the saliva levels for assessing the participants’ stress-related hormones cortisol and chromogranin A (Noto et al., 2005); posturography for assessing the participants’ balance and postural abilities (Visser et al., 2008); Timed Up and Go for assessing participants’ dynamic balance of lower extremity functions and mobilities (Podsiadlo & Richardson, 1991).
Characteristics of DMT Sessions
Most DMT interventions were conducted in group sessions (n=9, 90.0%), with only one (10.0%) conducted in individual sessions.
The intervention duration ranged from 30 to 60 minutes, with the most common intervention duration being 60 minutes (n=5, 50.0%). This was followed by 45 minutes, including 45 to 60 minutes (n=3, 30.0%).
The most frequent intervention frequency was once a week (n=5, 50.0%), followed by once every 2 weeks (n=2, 20.0%). Three (30.0%) studies did not report the intervention frequency.
The most frequent number of DMT intervention sessions was 10 (n=5, 50.0%), followed by less than 10 (n=2, 20.0%). Two studies (20.0%) did not report the intervention frequency.
Characteristics of Interventions (Elements of Activities)
The most common intervention method was a warm-up or introduction, development, and closing structure (n=5, 50.0%). Four studies (40.0%) did not report the structure of DMT interventions.
A total of 47 elements of activities were included in the DMT intervention. The most common elements of the activities in the DMT interventions were mirroring (n=5, 10.6%) and touching, including holding hands (n=5, 10.6%). The second most common element was authentic movement (n=4, 8.5%), and some types of dance (n=4, 8.5%) were also conducted. The next most common activities were the use of props (n=3, 6.3%) and expressing images (n=3, 6.3%) as movements.
Results of the Studies (Conclusion): Effects of DMT Interventions
There were 23 reports on the effectiveness of DMT interventions. The most common effects were improved balance (n=3, 13.0%; static balance, n=2; dynamic balance, n=1) and positive expression (n=3, 13.0%). The next most common effects were a decrease in attention and affective behaviors (n=2, 8.6%) and an improvement in body image (n=2, 8.6%), empathy (n=2, 8.6%), and self-cognition (n=2, 8.6%).
Results of Quality and LOE of DMT Intervention Studies
This study demonstrated that nine intervention studies were conducted from 1993 to 2024, and four studies (44.4%) were conducted in the past decade.
Regarding LOE, two studies (22.2%) were at level 2, three (33.3%) were at level 3, and four (44.4%) were at level 4. The study designs of level 2 of LOE were randomized controlled trials (RCTs) (n=2, 22.2%), whereas those of level 3 of LOE were before–after trials (n=2, 22.2%) and controlled clinical trials without RCTs (n=1, 11.1%). Level 4 of LOE were case study (n=1, 11.1%) and case series (n=3, 33.3%) (Table 2).
| Study design | LOE | Authors | Year | ||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |||
| Case study | 1 | Kozuka and Chino | (2008) | ||||
| Case series study | 1 | Shiba and Tanaka | (1993) | ||||
| 1 | Arakawa | (2000) | |||||
| 1 | Takahashi et al. | (2020) | |||||
| Before–after trials | 1 | Kaji et al. | (2000) | ||||
| 1 | Takahashi et al. | (2022) | |||||
| Controlled clinical trials without RCTs | 1 | Watanabe et al. | (2011) | ||||
| RCTs | 1 | Ishikawa et al. | (2014) | ||||
| 1 | Takahashi et al. | (2023) | |||||
| Total | 2 | 3 | 4 | ||||
LOE, levels of evidence; RCTs, randomized controlled trials.
Six (67.0%) of the nine intervention studies were based on study designs without control groups, such as a case study, and case series studies, and before–after trials.
Discussion
Japanese DMT intervention studies have been conducted since the establishment of the JADTA. However, the current status and quality of DMT intervention studies in Japan remain unclear.
This scoping review aimed to identify and review the literature regarding the participants, outcome measures, intervention methods, DMT intervention effect, and DMT intervention studies’ quality in Japan and synthesize information relating to the current status of DMT intervention studies in Japan.
The results of this study, based on databases and additional DMT journal search sources, indicated that nine studies met certain conditions of the search key terms.
Characteristics of Participants
In this study’s results, 99 of 169 DMT participants had some type of disease or disorder, and the participants’ diseases or disorders were diagnosed in 24 categories. The most common disease or disorder in DMT intervention studies in Japan was intellectual disability (n=42, 24.8%).
According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (American Psychiatric Association, 2022), intellectual disability is defined as “a disorder with onset during the developmental period that includes both intellectual and adaptive functioning deficits in conceptual, social and practical domains” (p. 37). Additionally, individuals with intellectual disability have defective motor function (Wuang et al., 2018).
DMT is expected to have a therapeutic effect on both intellectual and adaptive dysfunctions, which are characteristics of individuals with intellectual disability. Non-verbal physical communication interventions through DMT are characterized by their ability to intervene without language for individuals with intellectual disability. Thus, a unique feature of this intervention is that by implementing a non-verbal intervention, the intervention can be implemented even when the intellectual functioning of language skills is impaired (Takahashi et al., 2023).
In addition, mirroring or synchronizing movement interventions may enable individuals with intellectual disability to imitate or synchronize their movements with a therapist or the participants’ rhythm of movements in a DMT session, enabling them to learn appropriate behaviors in response to the situation (Takahashi et al., 2022). This may lead to decreased adaptive dysfunction.
Characteristics of Outcome Measures
In this study, only 13 (35.1%) of 37 outcome measures were standardized (n=6, 16.2%) and objective (n=7, 18.9%). Most DMT intervention studies in Japan used highly subjective outcome measures. This may be because, except for dance/movement therapists affiliated with universities and research institutions, numerous research practitioners have few opportunities to learn objective study methods. Additionally, these research implementers have limited opportunities to obtain research grants, making it difficult for them to purchase standardized outcome measures and objective measurement instruments.
However, the implementation of objective study methods is necessary to develop Japanese DMT. To conduct objective studies, regular study sessions between clinicians and researchers in each therapist’s area of expertise will deepen knowledge of studies and enable objective intervention studies. Additionally, conducting collaborative studies between clinicians and researchers or with other professionals may lead to the acquisition of research grants.
Characteristics of DMT Interventions (Elements of Activities)
The results indicated that the most common interventions were structuralized interventions (n=5, 50.0%), such as warm-up or introduction, development, and closing structure.
Marian Chace, the pioneer of DMT, created a structure of interventions that incorporated dance and movement as its prime communication and expression through three structures: warm-up (introduction), theme development (development), and closure (Levy, 2005). The purpose of each intervention was as follows (Levy, 2005): warm-up (introduction) aims to connect and communicate with participants during initial contact; theme development (development) aims to pick up, process, and reflect on participants’ thoughts, feelings, and ideas both verbally and non-verbally; closure aims to emphasize with participants a sense of release and satisfaction.
Most interventions (n=5, 50.0%) used the above structuralized interventions to achieve their objective. The implementation of structuralized intervention allows for the replication of studies. In addition, in a clinical setting, structuralized intervention is important to replicate the effectiveness of DMT intervention. Replicating the efficacy of DMT will enable its establishment as an effective therapy.
However, four interventions (40.0%) did not report any intervention methods. The description of the intervention is important to clarify its effects and should be described in future studies.
The most common elements of these activities were mirroring (n=5, 10.6%) and touching, including holding hands (n=5, 10.6%). When mirroring is used in conjunction with music as an intervention, the participants and therapist can link their movements, and through repeated imitation of the movements, improvements in balance abilities have been reported (Takahashi et al., 2020, 2023). Regarding touching, there have been no reports on specific procedures for utilizing touching in DMT interventions or their effects. Therefore, future studies should examine specific procedures for touching DMT interventions in Japan and their effectiveness in objective touching. Moreover, by demonstrating the specific use of touch, the characteristics of the DMT and its novel benefits in Japanese culture may become clear.
Results of the Studies (Conclusion): Effects of DMT Interventions
In this study, the most common effects were improved balance (n=3, 13.0%; static balance, n=2; dynamic balance, n=1) and positive expression (n=3, 13.0%). These effects suggest that DMT interventions in Japan can improve physical performance, improving the dynamic and static balance necessary for postural adjustment. The most frequent participants in DMT in Japan were individuals with intellectual disability, and the characteristic comorbidity was motor dysfunction. The study results may have been influenced by numerous reports indicating that DMT interventions have reduced motor dysfunction in the daily lives of individuals with intellectual disability.
In addition, through the DMT intervention in Japan, there was a mental improvement in positive expressions, which is necessary to maintain quality of life in daily life. Japanese DMT has therapeutic effects on both physical and mental health.
Quality and LOE of DMT Intervention Studies
The study results indicated that only two studies used RCT designs, and six were based on study designs without control groups, such as a case study, and case series studies, and before–after trials. Moreover, there were only two DMT intervention studies at level 2, three at level 3, and four at level 4. Based on these results, we found that levels of evidence in DMT intervention studies in Japan tended to be low.
The reasons for this are as follows. The DMT is characterized by reading participants’ thoughts and actions based on their facial expressions, communication, and physical expressions through movement and dance. It also includes selecting music, dances, and physical movements based on their characteristics. Although this allows therapists to read the changes in each participant and implement interventions tailored to each participant, it may be related to the difficulty of conducting an objective study design, such as RCTs. However, it is critical to provide a scientific rationale for DMT intervention studies to enhance the value of DMT in medical facilities, welfare areas, and educational facilities as therapeutic treatment, and an improved study design is essential.
For Future Studies
First, this study primarily focuses on DMT intervention studies conducted in Japan but also serves as a valuable reference for advancing scientific research and improving the quality of DMT protocols in intervention studies across other Asian countries with similar cultural elements and practices. By thoroughly analyzing the characteristics of DMT interventions in Japan, such as participants, intervention methods, treatment effects, and the quality of intervention studies, the DMT interventions that can be applied to other Asian countries are revealed. The results and data of this study may serve as a valuable reference for countries with similar cultural elements, providing specific guidelines and frameworks to enhance the quality of DMT protocols.
Second, although there are references introducing DMT practices in Asian countries such as China, Korea, Japan, Hong Kong, India, and Vietnam (Zhou et al, 2019), there has been no systematic review using objective research methods with high reliability and validity, such as Preferred Reporting Items for Systematic Reviews and Meta-Analyses. Consequently, the current status and quality of DMT intervention studies in these Asian countries remain unclear. Using this study as a reference to investigate the status of DMT intervention studies in Asian countries may clarify its effectiveness and challenges. Moreover, future research should compare Japanese DMT practices with those in other Asian countries to highlight distinctive features and understand their significance from an international perspective. This comparative approach could lead to improved protocols and a more nuanced understanding of DMT’s impact and effectiveness in diverse cultural contexts.
Third, we recommend that RCTs improve the quality of DMT intervention studies in Japan. In addition, we believe that the use of the Consolidated Standards of Reporting Trial (CONSORT) statement when conducting RCTs will ensure study quality. The CONSORT statement, comprising a 25-item checklist and flowchart, is an internationally established set of integrated standards for the reporting of clinical trials, aimed at improving the reporting of RCTs, helping readers understand the conduct of clinical trials, and evaluating the validity of trial results (Moher et al., 2010). Moreover, the use of standardized or objective outcome measures is essential to demonstrate the effectiveness of treatments based on scientific evidence.
Fourth, this study only represents the current status of DMT intervention studies in Japan; as the number of intervention studies increases, the characteristics of DMT in Japan may change. Therefore, further investigation will be necessary after several years.
Limitations
The first limitation is that very few DMT intervention studies are conducted in Japan, and the number of DMT intervention studies in Japan is limited. Among the excluded studies, the most common Japanese DMT studies were clinical reports (n=14; 27.4%). There have been some clinical reports on the current status of DMT intervention studies in Japan; however, these have not led to intervention studies. This may be because the Japanese DMT has not been defined, and specific treatments, such as intervention methods and therapeutic effects, may not be clear. Consequently, it is possible that the location of the study may be limited or that participants in intervention studies may not have been recruited. Although the number of selected studies was limited, this report is crucial for understanding the current state of DMT intervention studies in Japan.
Second, three selected studies (Takahashi et al., 2020, 2022, 2023) were authored by one of the authors of this study, which may have led to bias toward the results of this study. In addition, one study (Kaji et al., 2000) used two interventions and the same outcome measures for the two interventions, which may have biased the results of this study.
Conclusion
This study was the first attempt at a literature review of DMT intervention studies in Japan and focused on reviewing the literature using the PRISMA-ScR. This study revealed the following: There were only two studies at level 2 of EOL, and the levels of evidence in DMT intervention studies in Japan tended to be low; the most common disease or disorder was intellectual disability (n=42, 24.8%); the most common outcome measures were the Child Behavior Checklist (n=3, 8.1%), observing movements through recorded video (n=3, 8.1%), and Timed Up and Go (n=3, 8.1%). Only 13 (35.1%) of the 37 were used as standardized (n=6, 16.2%) and objective (n=7, 18.9%) outcome measures; the most used interventions were structuralized interventions (n=5, 50.0%), including mirroring (n=5, 10.6%) and touching, such as holding hands (n=5, 10.6%), as the elements of activities; the Japanese DMT conducted treatment effects for both physical and mental health.
This study can be used as a reference for protocol development to improve the quality of DMT intervention studies in Japan. It also may serve as a valuable reference for improving the quality of DMT protocols in intervention studies across other Asian countries with similar cultural elements and practices in future studies.
About the Authors
Hideki Takahashi, Ph.D., R-DMT, is a dance/movement therapist specializing in developmental support for children with and without developmental and neurodevelopmental disorders. He is currently affiliated with the Department of Pedology, Faculty of Human Life Science, Shikoku University. His research theme concerns developmental support for preschool-aged children, as well as motor and balance skills and adaptive behaviors in children with developmental and neurodevelopmental disorders.
Author to whom correspondence should be addressed; E-Mail: takahashi-hideki@shikoku-u.ac.jp; ORCID ID: https://orcid.org/0000-0001-8221-8561.
Yukari Sakiyama, Ph.D., BC-DMT, is a Certified KMP Analyst and Trainer. She currently serves as the vice president of the Japan Dance Therapy Association and is a research fellow at the Graduate School of Engineering, Mie University. Her ongoing research focuses on automating the KMP system, conducted within the Image Information Processing Laboratory in the Department of Electrical and Electronic Engineering, Information and Communication Systems Engineering at Mie University. E-Mail: sakiyama@mukogawa-u.ac.jp
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of Interest
The authors declare no conflict of interest.
References
Achenbach, T. M. (2015). Multicultural evidence-based assessment using the Achenbach System of Empirically Based Assessment (ASEBA) for age ½-90+. Psychologia: Avances de la Disciplina, 9(2), 13–23. | |
American Dance Therapy Association. (2020). American Dance Therapy Association. Retrieved March 10, 2025, from http://adta.memberclicks.net/ | |
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders: DSM-5 text revision (5th ed., pp. 37–45). American Psychiatric Association. | |
Arakawa, K. (2000). Dance/movement therapy with senile dementia patients: Movement and reminiscence functions. Japanese Journal of Dance Therapy, 1(1), 7–21. | |
Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19–32. | |
Çabalar, M., Selçuk, Ö., Yazar, T., Karamanli, Y., YetkJn, T., & Yayla, V. (2011). Rutin elektroensefalografide diken, keskin ve yavaş dalga aktivitelerinin anatomik lokalizasyonları / Anatomical localizations of spike, sharp and slow wave activities in routine electroencephalography. Medical Journal of Bakirköy, 7(3), 94–98. | |
Center for Evidence-Based Medicine. (2022). Explanation of the 2011 (OCEBM) levels of evidence. Retrieved June 28, 2022, from https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence | |
Ishikawa, Y., Tanaka, M., Musha, T., & Mizukami, K. (2014). Effects of dance therapy in elderly people with dementia. Nihon-Ninchishou-Yobou-Gakkai-shi, 3(1), 2–12. | |
Japanese Dance Therapy Association (JADTA). (2008). Certified by the Japan Dance Therapy Association (Nihon-dance-serapi-kyoukai-nintei) “Certification system manual (Shikakunintei-seido-setsumeisho)”. Retrieved September 5, 2023, from chrome-extension: //efaidnbmnnnibpcajpcglclefindmkaj/ https://jadta.org/wp-content/uploads/2020/03/shikaku-handbook-2020.pdf | |
Japanese Dance Therapy Association. (2023). Japanese Dance Therapy Association News. Japanese Dance Therapy Association News Letter, No. 150. | |
Jorm, A. F., Mackinnon, A. J, Christensen, H., Henderson, A. S., Jacomb, P. A., & Korten, A. E. (1997). The psychogeriatric assessment scales (PAS): Further data on psychometric properties and validity from a longitudinal study of the elderly. International Journal of Geriatric Psychiatry, 12(1), 93–100. | |
Kaji, M., Kouda, M., Yusa Y., & Hasegawa, M. (2000). The assessment of the efficacy of dance/movement therapy. Japanese Bulletin of Arts Therapy, 31(2), 42–52. | |
Kaufer, D. I., Cummings, J. L., Christine, D., Bray, T., Castellon, S., Masterman, D., Macmillan, D., MacMillan, A., Ketchel, P., & Dekosky, S. T. (1998). Assessing the impact of neuropsychiatric symptoms in Alzheimer’s disease: The Neuropsychiatric Inventory Caregiver Distress Scale. Journal of the American Geriatrics Society, 46(2), 210–215. | |
Keith, T. Z., Fine, J. G., Taub, G. E., Reynolds, M. R., & Kranzler, J. H. (2006). Higher order, multisample, confirmatory factor analysis of the Wechsler Intelligence Scale for Children–Fourth Edition: What does it measure? School Psychology Review, 35(1), 108–127. | |
Kozuka, T., & Chino, M. (2008). A study on dance therapeutic approach to the autistic child. Bulletin of the Integrated Research Center for Educational Practice, Utsunomiya University, 31, 33–40. | |
Levy, F. J. (2005). Dance movement therapy: A healing art (2nd ed., pp. 1–13, 19–27). Reston, VA: American Alliance for Health, Physical Education, Recreation and Dance. | |
Moher, D., Hopewell, S., Schulz, K. F., Montori, V., Gøtzsche, P. C., Devereaux, P. J., Elbourne, D., Egger, M., & Altman, D. G. (2010). CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. Journal of Clinical Epidemiology, 63(8), e1–e37. | |
Molloy, D. W., Alemayehu, E., & Roberts, R. (1991). Reliability of a standardized mini-mental state examination compared with the traditional mini-mental state examination. American Journal of Psychiatry, 148, 102–105. | |
Mukaide, S. (2020). Dance therapy as an Educational Support: Ibasho – “A Place Where One Feels Secure and Can Be Oneself” to engage with the self and the others. Japanese Journal of Dance Therapy, 13(1), 9–15. | |
Noto, Y., Sato, T., Kudo, M., Kurata, K., & Hirota, K. (2005). The relationship between salivary biomarkers and state-trait anxiety inventory score under mental arithmetic stress: A pilot study. Anesthesia & Analgesia, 101(6), 1873–1876. | |
Ohno, Y. (2014). Application of the dance therapy in two mental hospitals. Japanese Journal of Dance Therapy, 14(1), 25–30. | |
Ohnuma, Y., Sakiyama, Y., Machida, S., & Matsubara, Y. (2012). Dansuserapi-no-riron-to-jissen: Karada-to-kokoro-heno-hiiringu-aato. Chiyoda-ku, Tokyo, Jiaasu-kyouiku-shinsha. | |
Overall, J. E., & Gorham, D. R. (1962). The brief psychiatric rating scale. Psychological Reports, 10, 799–812. | |
Podsiadlo, D., & Richardson, S. (1991). The timed “up & go”: A test of basic functional mobility for frail elderly persons. Journal of the American Geriatrics Society, 39, 142–148. | |
Shiba, M., & Tanaka, A. (1993). On the practice and its evaluation of the dance therapy to psychiatric inpatients. Society for Mind-Body Science, 2(1), 37–47. | |
Stark, T., Walker, B., Phillips, J. K., Fejer, R., & Beck, R. (2011). Hand-held dynamometry correlation with the gold standard isokinetic dynamometry: A systematic review. American Academy of Physical Medicine and Rehabilitation, 3, 472–479. | |
Swain, D. P., & Leutholtz, B. C. (1997). Heart rate reserve is equivalent to %VO2 reserve, not to %VO2max. Medicine & Science in Sports & Exercise, 29(3), 410–414. | |
Takahashi, H., Seki, M., Matsumura, T., An, M., Sasai, T., Ogawa, Y., Matsushima, K., Tabata, A., & Kato, T. (2020). The effectiveness of dance/movement therapy in children with Williams Syndrome: A pilot study. American Journal of Dance Therapy, 42, 33–60. | |
Takahashi, H., An, M., Matsumura, T., Seki, M., Ogawa, Y., Sasai, T., Matsushima, K., Tabata, A., & Kato, T. (2022). Effectiveness of dance/movement therapy intervention for children with intellectual disability at an early childhood special education preschool. American Journal of Dance Therapy, 45, 20–40. https://doi.org/10.1007/s10465-022-09356-3 | |
Takahashi, H., An, M., Sasai, T., Seki, M., Matsumura, T., Ogawa, Y., Matsushima, K., Tabata, A., & Kato, T. (2023). The effectiveness of dance movement therapy for individuals with Down syndrome: A pilot randomised controlled trial. Journal of Intellectual Disability Research, 67(7), 640–654. | |
Tombaugh, T. N., & Mclntyre, N. J. (1992). The mini-mental state examination: A comprehensive review. Progress in Geriatrics, 40, 922–935. | |
Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac., D., Moher, D., Peters, M. D. J., Horsley, T., Weeks, L., Hempel, S., Akl, E. A., Chang, C., McGowan, J., Stewart, L., Hartling, L., Aldcroft, A., Wilson, M. G., Garritty, C., Lewin, S., Godfrey, C. M., Macdonald, M. T., Langlois, E. V., Soares-Weiser, K., Moriarty, J., Clifford, T., Tunçalp, Ö., & Straus, S. E. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Annals Internal Medicine, 169(7), 467–473. | |
Tsushima, E. (2017). Design and statistical method in clinical research of physical therapy. Physical Therapy Japan, 44(6), 463–469. | |
Tulsky, D. S., Saklofske, D. H., Wilkins, C., & Weiss, L. G. (2001). Development of a general ability index for the Wechsler Adult Intelligence Scale—Third Edition. Psychological Assessment, 13(4), 566–571. | |
Visser, J. E., Carpenter, M. G., Kooij, H. V. D., & Bloem, B. R. (2008). The clinical utility of posturography. Clinical Neurophysiology, 119, 2424–2436. | |
Watanabe, A., Ukon, M., Moriyama, T., Tamura, S., Asaka, T., & Inoue, K. (2011). Psycho-physiological effects of group dance/movement therapy on frail elderly women attending day-care centers of geriatric health services facilities. Bulletin of Hokkaido Bunkyo University, 35, 93–103. | |
Wuang, Y. P., Wang, C. C., Huang, M. H., & Su, C. Y. (2018). Profiles and cognitive predictors of motor functions among early school-age children with mild intellectual disabilities. Journal of Intellectual Disability Research, 52(12), 1048–1060. | |
Yamaguchi, M., Kanemori, T., Kanemaru, M., Takai, N., Mizuno, Y., & Yoshida, H. (2004). Performance evaluation of salivary amylase activity monitor. Biosensors and Bioelectronics, 20, 491–497. | |
Zhou, T., Kim, N., Machida, S., Sakiyama, Y., Tsai, P.-S., Lee, T., Hung Ho, R., Bijlani, R., Mehta, D., & Bui, M. (2019). Dance movement therapy in Asia: An overview of the profession and its practice. Creative Arts in Education and Therapy, 5(1), 40–50. |





